




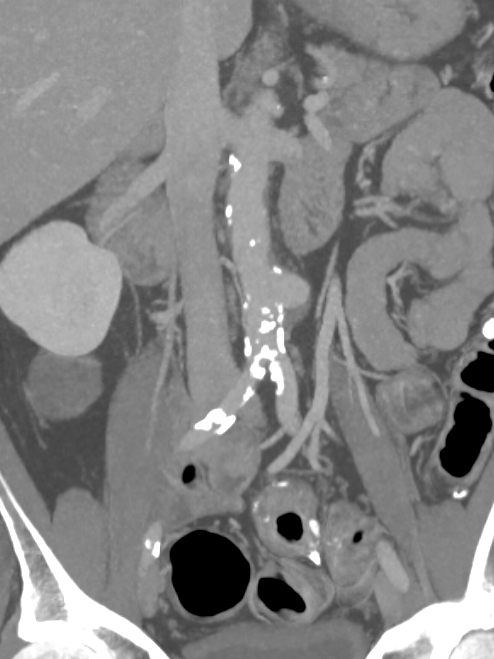
Angiograms showing vascularity of the lesion. The two annotated images show the tortuosity of the vessel supplying the lesion. The dotted orange coloured line shows the path of the vessel. It was not possible to cannulate this artery with conventional microcatheters.


Adequate catheter position attained using the Swift Ninja Catheter by Merit Medical. Final image showing reduced vascularity.







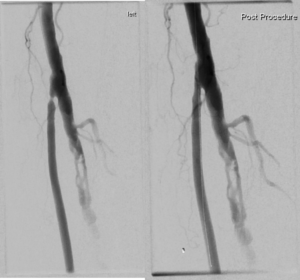


 Two weeks later represented acutely with thrombosed graft. Due to underlying problems with the graft decision made to attempt to re-canalise the native arteries.
Two weeks later represented acutely with thrombosed graft. Due to underlying problems with the graft decision made to attempt to re-canalise the native arteries. Triphasic flow is seen on Doppler three months later.
Triphasic flow is seen on Doppler three months later.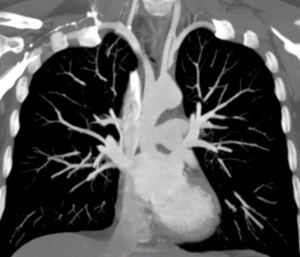
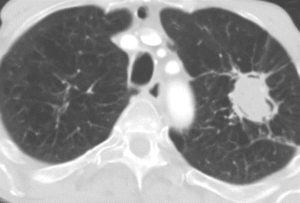
 CT shows likely embolic disease in the left subclavian artery. There is high risk of further distal embolisation to hand or cranial embolisation via the left vertebral artery.
CT shows likely embolic disease in the left subclavian artery. There is high risk of further distal embolisation to hand or cranial embolisation via the left vertebral artery.